
The Good Gut Guide: Help for IBS, Ulcerative Colitis, Crohn's Disease, Diverticulitis, Food Allergies and Other Gut Problems
The
Good Gut
Guide
Help for IBS • Ulcerative Colitis
Crohn’s Disease • Diverticulitis
Food Allergies • Other Gut Problems
Stephanie Zinser
Foreword by Professor R. John Nieholls

Contents
Cover
Title Page
Excerpt
Foreword
How I Came to Write This Book
Introduction
SECTION 1
Having trouble with your guts?
What it means and what you can do about it
CHAPTER 1
A quick anatomy lesson
CHAPTER 2
Common symptoms
Constipation
Diarrhoea
Nausea
Bleeding
Mucus
Abdominal pain
Pain in the back passage
Wind and bloating
Urgency, frequency and incomplete evacuation
Itchy bottom
CHAPTER 3
How to get the best from your doctor
CHAPTER 4
Investigating the problems – a look at tests, scans and ’scopes
SECTION 2
The medical possibilities
CHAPTER 5
How lifestyle can affect the digestive system
Drinking too much alcohol
Stress
Athlete’s diarrhoea
Changes in routine
Ignoring the urge to go
Talting antibiotics
(Over)use of aspirin
Prescription and non-prescription drugs
CHAPTER 6
How diet and nutritional problems affect the digestive system
Chronic dehydration
Caffeine
Fibre
Strongly coloured foods and ‘false’ bleeding
Inadequate nutrition through malabsorption
Food allergy and intolerance
Lactose intolerance (hypolactasia)
Coeliac disease
CHAPTER 7
How problems of the reproductive system can affect your guts
Period pains
Constipation during pregnancy
Chlamydia
Endometriosis
Ovarian cysts
Ovarian cancer
Toxic shock syndrome (TSS)
CHAPTER 8
The thyroid and its effect on the digestive system
Underactive thyroid (hypothyroidism)
Overactive thyroid (hyperthyroidism, Graves’ disease)
CHAPTER 9
Infectious illnesses of the digestive tract
Bacterial food poisoning
Viral gastroenteritis
Protozoan parasitic infections: giardiasis, amoebiasis (amoebic dysentery) and cryptosporidiosis
Parasitic worm infestations
Tropical worm infestations
Botulinum poisoning
Typhoid/paratyphoid
Cholera
CHAPTER 10
Adhesions and hernias
Adhesions
Hernias
CHAPTER 11
Pains in the butt – haemorrhoids, fissures and others
Haemorrhoids (piles)
Pruritus ani
Anal abscesses
Anal fistulas
Anal fissures
Rectal prolapse
CHAPTER 12
Irritable bowel syndrome or (IBS)
CHAPTER 13
Inflammatory bowel disorders (IBDs)
Ulcerative colitis (UC)
Crohn’s disease
The IBD detectives: looking at clues
CHAPTER 14
Other inflammatory gut conditions
Gastritis
Peptic ulcers (gastric and duodenal ulcers)
Proctitis
Diverticular disease
CHAPTER 15
Emergency conditions
Appendicitis
Peritonitis
Intestinal obstruction or intestinal blockage
CHAPTER 16
Cancers and growths
Polyps
Colorectal (large bowel) cancer
Stomach or gastric cancer
Anal cancer
CHAPTER 17
Childhood gut problems
Threadworm (pinworm)
Encopresis
Intussusception
CHAPTER 18
Hospitals, surgery and more …
Hospitals
Being Stitched Up: Abdominal Surgery
When things don’t quite go according to plan
Me and my bag
I’m a kangaroo! Living with an internal pouch
SECTION 3
The person behind the illness
CHAPTER 19
A look at depression
CHAPTER 20
Coping
Coping with flare-ups: living a normal life
Coping with strange reactions
Coping with a partner: sexuality and the passion killers
CHAPTER 21
The future for gut health
If I had a crystal ball …
Probiotics – bugging us back to health?
A resource tool – self-help and other associations, websites and further information
Index
Acknowledgements
Copyright
About the Publisher
Excerpt
A man goes to his doctor with a piece of lettuce sticking out of his bum. He tells the doctor that he is a little concerned. After examining him, the doctor sighs and says, ‘I’m afraid it’s worse than I first thought … that’s just the tip of the iceberg.’
Foreword
In the last 20 years an increasingly informed public has acquired considerable medical knowledge. This has come through printed media, television and the Internet – and by contact with health care professionals like doctors and nurses.
People working in medicine who understand the need for greater communication often find this terribly rewarding. Taking time to explain, honestly, the good and bad aspects of managing illness should nowadays be an essential part of every consultation between the patient and their doctor.
Everybody, including patients and their relatives, wants to know more about their health. The Good Gut Guide deals with intestinal diseases. Although this may at first seem to be a small part of the totality of medicine, intestinal diseases and problems are in fact very common. For example, Irritable Bowel Syndrome is one of the most frequent reasons for seeing a GP. While the condition is not life-threateningly serious, it accounts for a huge amount of suffering and has economic consequences because of time taken off work. Other intestinal diseases also have a great impact on individuals and society: infections, inflammatory bowel diseases such as ulcerative colitis and Crohn’s disease, and cancers are all disabling – whether temporarily or more chronically – to millions of people.
Inflammatory bowel diseases affect young people. In some cases they can be very severe but in most, medical and surgical treatment can keep them under control, allowing the patient to lead a normal life. Bowel cancer is the second most common malignancy in our society, yet if diagnosed early it is curable. Polyps can give us early warning. These are tumours in the benign stage, and if removed, there is every chance that their evolution into cancer can be avoided. Indeed, cancer prevention by appropriate screening, increasingly through genetic indicators, offers a real opportunity for doctors to improve the results of cancer treatment.
Anal problems are extremely common. Although not serious, piles, abscesses and ulcers such as fissures can make life miserable for millions of sufferers. Incontinence may make life impossible, confining sufferers to staying at home near the toilet, too fearful to venture out to the shops let alone to social occasions such as parties or family gatherings. The good news is that these diseases are almost always treated successfully.
The Good Gut Guide is an impressive creation. It covers a vast field and includes just about every area that can be related to the intestine. It is accurate, well informed, practical and readable. It gives the medical facts in an authoritative and balanced manner and, at the same time, offers vital advice on the holistic aspects – such as diet and lifestyle – that are not usually available in normal medical books.
It will help patients and anyone else who wants to learn more about intestinal problems and improve their gut health.
PROFESSOR JOHN NICHOLLS
How I Came to Write This Book
When I first started suffering with proctitis in 1987, I was told it was a mild and localized form of ulcerative colitis, which was very unlikely to become serious or ever result in major surgery. Unfortunately, I was one of the unlucky few and 11 years later my entire large bowel was removed during a complex and lengthy operation.
It was very painful but, at the age of 34, I was more concerned about the prospect of wearing a ‘bag’ for the rest of my life. I mistakenly believed I’d have to wear baggy clothes and would never be able to enjoy scuba diving, swimming, or even lying on a beach again. However, I was given an ‘internal pouch’ instead. This involved reconfiguring my intestines to make part of my small bowel into a reservoir for digestive waste, meaning that I could continue to ‘go to the bathroom’ almost as normal. I thought it was great (despite a few practical limitations and the odd bout of ‘pouchitis’) – not only did it enable me to live without self-consciousness, I was finally free of my UC. I was bursting with energy and enthusiasm.
Having spent the better part of 10 years explaining my illness to people, I was amazed at how taboo the subject of bowels was. We seemed to be at the same stage of ignorance and silence that breast cancer sufferers were 30 or 40 years previously – when women were too ashamed to go to their doctor with a breast lump and when they, quite literally, died because of their embarrassment. But look at how all that has changed – with massive health and charity campaigns raising public awareness of this terrible illness.
I wanted to see the same revolution for sufferers of bowel diseases. So, just days after leaving hospital, I made an impulsive call to the Daily Mail’s Good Health Editor at the time, Rory Clements. Despite having never written for publication before, I offered to write him an article on my experience. Amazingly, he took up my offer and the full-page feature was duly published in March 1998. It marked the start of my efforts to take the taboo out of bowel illnesses.
So why write this book now? For the same reasons I made that phone call. Statistically, you are more likely to be killed by a donkey than not suffer with some gut-related problem at some time during your life. Many gut problems – including bowel cancers – are more easily and more successfully treated when they’re picked up early. Taboos often prevent people from addressing problems until they are just too big and too serious to ignore, by which time it may be too late. Talk destroys taboos. Information saves lives.
I hope this book will help us to destroy the taboo, and enjoy good gut health.
Introduction
When I was 25 years old I experienced a disturbing symptom – bleeding from my bottom. Because I was then pregnant, I put it down to simple haemorrhoids and thought nothing more of it.
I never suspected that this was the beginning of a decade’s worth of increasingly serious illness that I would face virtually alone, unaided and only vaguely informed. It wasn’t the doctors’ fault – they told me what, medically, I needed to know. And there were support groups, although I tended to notice only the people who suffered far worse than I did. Because of this, I shied away from associating with them – as if the seriousness of their illnesses might somehow be contagious.
Things that go wrong with your guts cause great embarrassment and this in turn makes them frightening. You don’t automatically know who to talk to or what words to use, and when you do seek medical help the resulting procedures can be embarrassing as well as uncomfortable.
For some reason bowel and intestinal disorders have always been viewed as older people’s afflictions, despite the fact that most cases of ulcerative colitis (UC), Crohn’s disease and IBS start during a person’s mid-twenties (or younger) – when many people are single, embarking on relationships, starting families or juggling demanding careers and busy social lives. I’m not sure why this false image has so stubbornly persisted, although I believe it is slowly changing.
As a health writer, I am regularly bombarded by information about new treatments – not just from orthodox medicine, but also from the herbal, dietary and complementary sides. My personal view is that the key to a ‘golden cure’ is not the preserve of any one of these camps. The answer to bowel illnesses is probably (and quite unsatisfactorily for those of us who like things neat and tidy) a complicated mixture of several elements, the proportions and exact ingredients of which we simply cannot isolate today. It’s up to us to look carefully at every possibility, to try whatever we feel may be right for us, and work toward the best possible outcome – good gut health.
And that’s why I’ve written this book – to provide the appropriate information so that the reader can play an active role in achieving good gut health. It isn’t a book that features only a couple of gut problems in great detail. Neither is it a medical encyclopaedia that covers a whole raft of illnesses on a basic level. It is a user-friendly book for anyone who has ever experienced gut problems – and one that discusses them in a way that people understand.
This book looks at all types of intestinal symptoms – like diarrhoea, wind, constipation, nausea, abdominal pain and more – and offers practical solutions for dealing with them. Not just medical solutions, but self-help – including dietary and lifestyle tips, herbal help and a whole range of complementary therapies, from flower remedies to Ayurveda (an ancient Indian system of medicine). This approach is vital. People today are more proactive in choosing their healthcare than ever before and it is important to me that this book strongly reflects the diverse range of options now available.
Having looked at symptoms, the book then homes in on the diseases that are the key culprits of gut trouble and explains, simply but in detail, what these diseases are, what causes them, who they typically affect, what the risk factors are, how to prevent them and what medical treatments are available. Again, I have included practical advice for the patient in terms of self-help, dietary management, alternative treatments and prevention.
Lastly, the book focuses on the person behind the illness. It looks at the effect that chronic or embarrassing illnesses can have on our daily lives, our personalities and our relationships. It offers advice on the practicalities of living a normal life and coping with depression, hospitals, illness and surgery. There is also a large resource section at the back of the book for anyone who wants access to support groups, medical agencies and further information.
SECTION 1
having trouble with your guts?
What it means and what you can do about it
Anything unusual that happens to our guts – like rampant diarrhoea or sudden bleeding – is disturbing. However, such occurrences are not the only reason we visit our doctor with a gut-related problem. Some common conditions like constipation are often mild, but they may gradually worsen until we become concerned enough to seek medical advice. You can just as easily need to see your doctor for a chronic problem as an acute one.
There are hundreds of medical problems – serious as well as minor ones – that cause ‘gut-related’ symptoms such as diarrhoea, constipation or mild stomach pains. This makes symptoms tricky to assess. How do we know when they are serious enough to warrant medical advice? Very few people get a thrill from visiting their doctor to be told that they are making a fuss but, on the other hand, what would happen if we ignored something serious?
Most digestive problems, whether serious or commonplace, don’t present just one symptom. Usually we notice a couple, perhaps more. Here’s an example: George notices that he’s constipated, and occasionally sees flecks of bright red blood on the toilet paper; Sally feels a lot of discomfort when she goes to the toilet, especially when she is straining, and is also irritated by anal itching. George and Sally each have piles. They have the same condition, but they have differing symptoms. George’s main problems are constipation and bleeding, Sally’s are discomfort and itching. This is another reason why it is sometimes difficult to tell what is causing a particular health problem.
Analysing your symptoms in an almost detached way is part of the answer. For this reason, Section 1 focuses on the common symptoms like diarrhoea, constipation, bleeding, and wind and bloating. Very few of us wake up and think, ‘I think I’ve got inflammatory bowel disease.’ More likely we’ll say, ‘This diarrhoea is getting me down, I wonder what’s causing it and how I can stop it.’ This section explains what can cause these symptoms and offers a variety of practical ways we can help relieve them.
Section 1 also discusses how we can get the best from our doctors – by knowing what to ask, how to ask and what to expect from medical consultations, and describes the major tests that are used by doctors to explore and identify gut problems.
CHAPTER 1
A Quick Anatomy Lesson
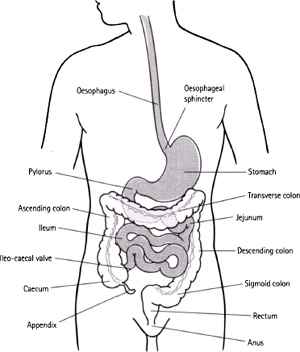
First, let’s go back to the classroom. It is easier to understand why things go wrong – and how we are affected – if we know a little about the anatomy of the gut.
The digestive system starts at our mouth and ends up at the other end – the anus. When people talk about ‘guts’ they can mean pretty much anything, from the throat to the stomach to the intestines, although generally, most people think of the stomach and the small and large intestines when they say ‘gut’. Vagueness may be okay when we’re chatting with friends, but there’s little room for it in the doctor’s office. Being specific helps our doctors understand what we’re talking about. We might think we’re being fairly exact when we say ‘abdominal’, but a doctor could easily wonder whether we mean the stomach, the small intestines or the large bowel (colon and rectum). And should he ask which it is, it helps to know what he’s talking about.
A few minutes spent looking at the drawing overleaf should help. This shows the whole digestive system, its various parts and their medical names. The other diagrams provide a little more detail about the lining of the intestines. There are different layers, each of which performs different functions. The whole of the digestive system is hugely vascular (that is, rich in blood vessels). A staggering quantity of blood passes through it – some 40 per cent of our blood supply is diverted through the digestive system after a meal, so that the blood can absorb the goodness our food delivers to our bodies. That’s why it isn’t a good idea to embark on strenuous exercise soon after eating – it puts too many demands on our body systems.
The Mouth to the Oesophagus
The mouth is the first organ of digestion. Teeth chew our food, physically breaking it down, and the inside of our mouth contains glands that produce saliva – not only when we eat food but also when we’re just thinking about it. Saliva is important. This liquid, which is neutral to slightly acidic, not only starts the chemical process of digestion, but it lubricates each mouthful, helping us to swallow properly. We produce about 1.7 litres (about 60fl oz) of saliva every day. One of the main enzymes contained in saliva is called amylase, which starts breaking starch down into more basic sugars. When we swallow, food enters the first ‘tube’ – the oesophagus, which is about 25cm (10in) long. The oesophagus doesn’t do anything to digest food. Waves of muscle contraction (called peristalsis) help push the food down the oesophagus. These muscular contractions are so strong that you can drink a glass of water while standing on your head.
The Stomach
Food enters the stomach through a ring of muscle (sphincter) that prevents the stomach contents from travelling back up the oesophagus – the one normal exception to this is during vomiting. The stomach is so stretchy that it can hold up to 2 litres (about 70fl oz) of fluid. While food is in the stomach it is subjected to both physical and chemical action. Stomach acids – mostly hydrochloric acid (one of the strongest acids known to man) – reduce the stomach contents to a porridge-like consistency, while the stomach also mechanically ‘churns’ the food during the four hours or so that food stays there. Because the stomach contents are very acidic, we get ‘burning’ sensations when we vomit, have indigestion or gastric reflux, as the contents bubble back up into the oesophagus. After a while, the sphincter muscle (called the pylorus) that holds the lower end of the stomach closed starts to relax, allowing the partly-digested food to trickle out into the first portion of the small intestine.
The Small Intestine
As food is squirted through the pylorus, it enters the first part of the small intestine, the duodenum. Here, more digestive chemicals are introduced, further breaking down the food. Bile, for example, an alkaline substance that is made in the liver, is pumped out by the gall bladder when needed. Bile acts as a detergent and emulsifying agent, breaking fats down into small droplets. Pancreatic enzymes break down carbohydrates and proteins: amylase acts on carbohydrates and trypsin and chymotrypsin help digest proteins. Fats are also further broken down by lipase, another pancreatic enzyme.
The next section of the small intestine, the 3 metre (10ft) long jejunum, is where most of the nutrients released from food start to be absorbed. The walls of the jejunum are completely covered with tiny finger-like projections called villi. Millions of these millimetre-high folds line the intestinal walls, their purpose being to massively increase the surface area to make absorption of nutrients into the bloodstream effective (see figure overleaf). If the small intestines didn’t have villi, they would need to be about 2 miles long to do the same job – in fact, they are only about 6 metres (20ft) long. After the jejunum comes another 3 metre (10ft) long section of small bowel commonly known as the ileum. Although there are still many villi here, there are fewer than in the jejunum. The ileum continues to absorb nutrients into the bloodstream, but the focus here is more on water and salts; as food progresses through the small bowel, the consistency of it becomes thicker and more ‘sludgy’. In the very last part of the ileum, vitamin B12 is absorbed.